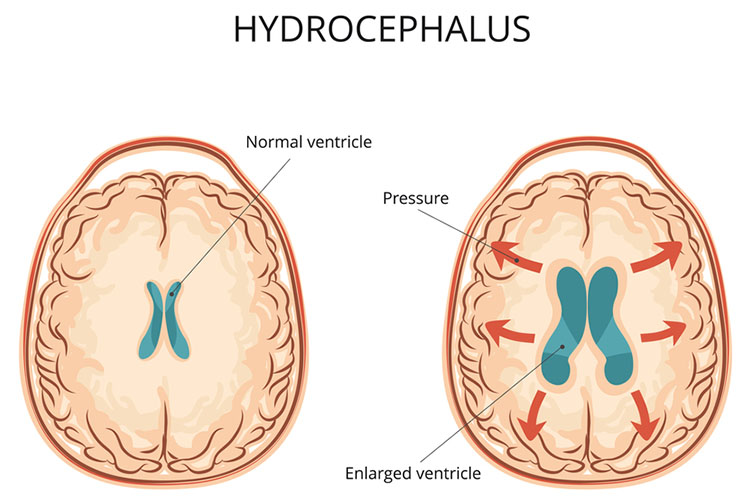
Hydrocephalus is a condition in which there is an accumulation of cerebrospinal fluid (CSF) in the ventricles, increasing the intracranial pressure within the skull (NINDS 2023).
Hydrocephalus can be caused by a variety of different diseases and injuries, including those that cause disruptions to the absorption of CSF or an obstruction to the CSF flow (Koutoukidis et al. 2016).
There are different treatments available for those with hydrocephalus depending on the individual, but they often involve the insertion of a shunt.
A shunt allows the excess CSF to drain to a different part of the body. In the older patient with idiopathic normal pressure hydrocephalus, insertion of a ventriculoperitoneal (VP) shunt shows improvement rates in 61 to 90% of patients presenting with this condition (Saehle et al. 2014). Idiopathic normal pressure hydrocephalus is often diagnosed in older adults and is characterised by gait disturbances, cognitive impairment and urinary incontinence (Cleveland Clinic 2022).
Different Types of Shunts
The different types of shunts used most commonly include ventriculoperitoneal (VP) shunts, ventriculoatrial (VA) shunts and lumboperitoneal (LP) shunts (Koutoukidis et al. 2016).
Shunts will generally consist of three components:
An inflow catheter - This drains the CSF from the ventricles. It leaves the brain through a small hole in the skull, which then runs under the skin.
A valve mechanism - This regulates the pressure control through the shunt tubing. It is connected to the catheter and lies between the skin and the skull, usually on top of the head or behind the ear.
A distal catheter - This runs under the skin and moves the CSF from the valve to the peritoneal cavity, heart or another drainage site.
(Hydrocephalus Association 2023a)
As with any procedure, every shunt and every person with a shunt is different. What works for one person may not necessarily be ideal for the next. This is why some valves can be adjustable, meaning that instead of having a fixed pressure valve at the same value for everyone, these adjustable valves can be readjusted by a clinician according to patient need (Hydrocephalus Association 2023a).
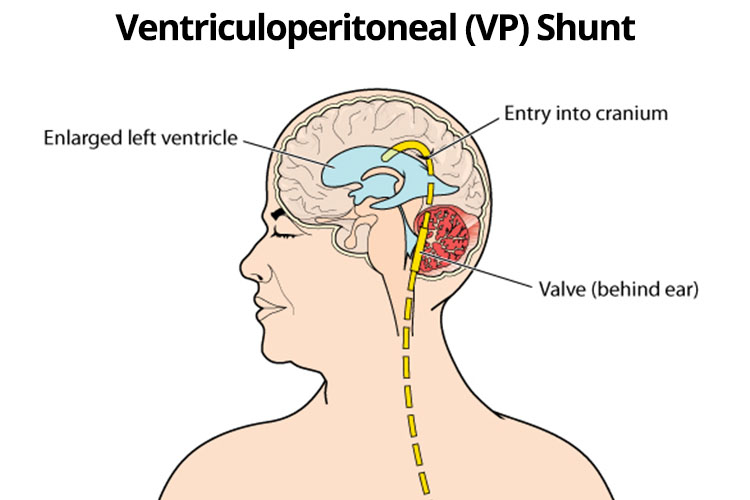
Ventriculoperitoneal (VP) Shunt
VP shunts are the most common type of shunt for draining excess CSF. These shunts generally contain a pressure-sensitive valve that releases CSF once the pressure reaches a certain level (Rinker et al. 2015). In VP shunts, a catheter is inserted into the ventricle with tubing tunnelled subcutaneously down the thorax and then further tunnelled into the peritoneal cavity where the CSF is absorbed.
Ventriculoatrial (VA) Shunt
VA shunts are less common than VP shunts and fairly similar. The only difference is that rather than finishing in the peritoneal cavity, the VA shunt finishes in the right atrium of the heart and CSF is absorbed via the bloodstream (Rinker et al. 2015).
Lumboperitoneal (LP) Shunt
An LP shunt consists of a catheter inserted between two lumbar vertebras into the thecal space, which is then tunnelled around the abdomen into the peritoneal cavity for absorption (Rinker et al. 2015).
Complications of Shunts
As with any surgery, the insertion of a shunt doesn’t come without risks. These risks include mechanical obstruction of the shunt, infection and subdural haematomas.
These complications can be divided into two categories as either arising from:
A mechanical complication
A biological complication.
Mechanical complications of a shunt include malfunctions such as leakage, obstruction, migration or discontinuity.
Examples of biological complications of a shunt include infection, haemorrhage, haemotoma and seizures (Fowler et al. 2023).
The complication rates following insertion of a shunt tend to be high, with up to half of patients experiencing some type of complication and requiring shunt revisions. Generally, with these complications, there is often an overlap of both biological and mechanical factors causing the problem (Rinker et al. 2015; Saehle et al. 2014).
Shunt blockages occur in up to 31% of patients and over drainage occurs in about 3% of patients (Chari et al. 2014).
Over drainage from the shunt can result in the ventricles decreasing in size and their meninges pulling away from the skull. This is a condition often called slit-ventricle syndrome. This complication is more common in young adults who have had a shunt in place since childhood. Someone with slit-ventricle syndrome will often complain of severe but intermittent headaches that are often only relieved when lying down (Hydrocephalus Association 2023b).
Under drainage of shunts has the opposite problem and will cause the ventricles to increase in size. This will be in conjunction with the individual also not experiencing any relief of their previous symptoms of hydrocephalus. When this occurs, the patient may need a revision of their shunt, or if the person is able to adjust their pressure valves externally, these will need to be reviewed and readjusted (Hydrocephalus Association 2023b).
Shunt infection tends to be one of the most common biological complications that occur. This can be quite significant, as infection may have further implications and detrimental effects on the individual, including abscess formation or shunt occlusion. If infection occurs, the shunt will generally need to be revised (Rinker et al. 2015).
Peritonitis can also occur with VP shunts, causing the individual to display general signs and symptoms of infection in conjunction with abdominal pain.
When a patient with a VP shunt complains of abdominal pain, the formation of an abdominal abscess also needs to be excluded. These abscesses may occur in many different ways, including shunt contamination or shunt migration into the bowel (Rinker et al. 2015).
A CSF pseudocyst is a rare complication of VP shunting with an unclear cause. It will generally develop some time after the shunt has been placed - sometimes up to years down the track (Rinker et al. 2015).
VP shunts can also become obstructed. This may be due to the catheter disconnecting, migrating or even fracturing (Rinker et al. 2015). The shunt may become blocked in any part, from the ventricular catheter in the brain to the distal part of the catheter where it is draining (Hydrocephalus Association 2023b).
Symptoms of a VP shunt obstruction are those seen with increased intracranial pressure, which could include headache, vomiting, lethargy, irritability and confusion (Koutoukidis et al. 2016).
Nursing Care of a Patient with a Shunt
Nurses need to monitor a patient with a shunt for any of these complications. If they suspect any of these complications are occurring, they need to act immediately, as a delayed response can have dire consequences for the patient.
It is also important to note that some of these complications can occur at any time. If your patient has had a shunt for five years, they can still be at risk of complications. Never stop monitoring for complications.
Topics
References
Chari, A, Czosnyka, M, Richards, HK, Pickard, JD, Chir, M, Czosnyka, ZH 2014, ‘Hydrocephalus Shunt Technology: 20 Years of Experience from the Cambridge Shunt Evaluation Laboratory’, Journal of Neurosurgery, vol. 120, no. 3, pp. 697-707, viewed 12 October 2020, https://thejns.org/view/journals/j-neurosurg/120/3/article-p697.xml
Saehle, T, Farahmand, D, Eide, PK, Tisell, M & Wikkelso, C 2014, ‘A Randomized Controlled Dual-center Trial on Shunt Complications in Idiopathic Normal-pressure Hydrocephalus Treated With Gradually Reduced or Fixed Pressure Valve Settings’, Journal of Neurosurgery, vol. 121 no. 5, viewed 6 October 2023, https://thejns.org/view/journals/j-neurosurg/121/5/article-p1257.xml
For Teams
Assign to your staff
Assign mandatory training and keep all your records in-one-place.
 New
New