Cutaneous Squamous Cell Carcinoma (cSCC): Dysplasia to Invasion
CPDTime.
10m
Updated 02 Aug 2023
Cutaneous squamous cell carcinoma (cSCC) is the second-most common type of skin cancer after basal cell carcinoma (BCC), accounting for about 33% of skin cancers (Cancer Council Victoria 2022).
While cSCC is a less serious form of skin cancer than melanoma, it can grow quickly and spread, causing potentially serious complications if untreated (Cancer Council Victoria 2022; Mayo Clinic 2021).
However, If addressed early, cSCCs can be easily resolved in most cases (Hale & Hank 2023).
cSCC has several features distinguishing it from BCC and melanoma. Awareness of these differences can assist with timely referral and treatment, thereby reducing morbidity associated with aggressive tumours and enhancing overall patient outcomes. All healthcare professionals should be able to identify lesions and refer appropriately.
What is Cutaneous Squamous Cell Carcinoma?
cSCC is triggered by DNA mutation (caused by UV radiation or other factors) to the flat cells located in the upper layer of the epidermis, known as squamous cells. This mutation causes the squamous cells to grow and divide abnormally. cSCCs grow quickly over weeks or months (Cancer Council Victoria 2022; Hale & Hank 2023; Healthdirect 2023).
Squamous cells can be found in many parts of the body, all of which are susceptible to developing cSCC. However, in most cases, cSCCs appear on areas of skin that are most frequently exposed to UV radiation (Healthdirect 2023). These include:
Face
Lips
Hands
Ears
Forearms
Lower legs.
(Oakley 2015)
Bowen’s disease is a pre-cancerous form of cSCC that generally presents as a red, scaly patch. If unaddressed, it may develop into cSCC (Healthdirect 2023).
Note: While ‘cutaneous squamous cell carcinoma’ specifically refers to cancer of the skin, squamous cell cancers can also develop internally (e.g. in the mouth, throat or lungs). These are known as squamous cell carcinoma (SCCs) (Hale & Hank 2023).
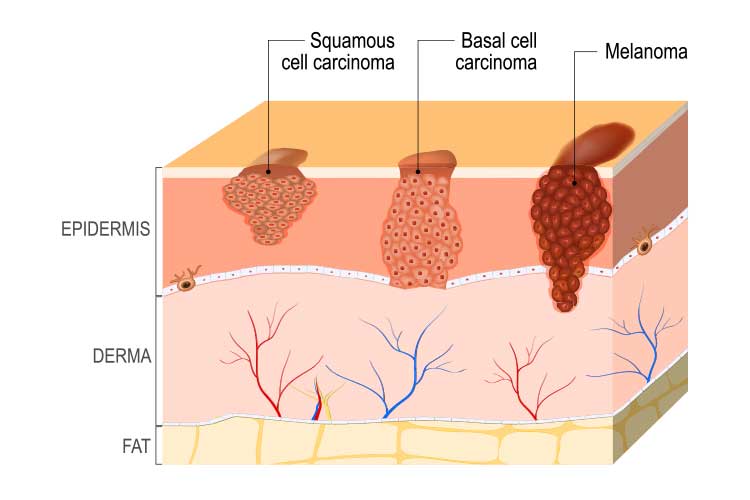
Cutaneous Squamous Cell Carcinoma v Basal Cell Carcinoma v Melanoma
Location of origin
Common physical characteristics
Growth and spread rate
Image
cSCC
Squamous cells (upper layer of the epidermis)
Thickened red, scaly or crusted spot
There may be bleeding or inflammation
Grow and spreads quickly; generally not serious but can cause complications if untreated.
BCC
Basal cells (bottom layer of the epidermis)
Red, pearly or pale lump
May be shiny or dry and scaly
Grows slowly and is unlikely to spread; least serious type of skin cancer.
Melanoma
Melanocytes (pigment-making cells in the epidermis)
Can be a new spot, or an existing one that begins to change
Flat or raised with irregular edges
May be more than one colour (brown, black, blue, red, white, light grey, pink or skin-coloured)
Grows and spreads quickly; most serious type of skin cancer.
(Cancer Council Victoria 2022; ACS 2019; SunSmart 2014)
Prevalence of Cutaneous Squamous Cell Carcinoma
There are over one million treatments performed anually for non-melanoma skin cancers in Australia. SCCs most commonly affect people over the age of 50 (Cancer Council Victoria 2022).
cSCC and BCC combined cause about 560 deaths annually (CCA 2019).
Risk Factors for Cutaneous Squamous Cell Carcinoma
Being male
Being over the age of 50
Fair complexion (particularly if the individual has freckles, blonde or red hair or blue or green eyes)
Direct ultraviolet (UV) exposure (either from the sun or artificial sources)
History of sunburns
Reduced immune function due to illness or immunosuppressive medications
Exposure to ionising radiation or chemical carcinogens
Human papillomavirus (HPV) infection
Individual response to chronic inflammation (such as a burn site)
Certain genetic disorders such as xeroderma pigmentosum.
(Hale & Hank 2023; Mayo Clinic 2021)
About 90% of cSCC cases can be attributed to UV exposure (Hale & Hank 2023).
Warning Signs of Cutaneous Squamous Cell Carcinoma
There are a number of signs to look for when identifying potential cSCCs, as they can present in a variety of ways. Surface changes may include:
Thick, red, scaly patches that may bleed or crust
Raised growths or lumps, possibly with a depression in the middle
Raised areas or new sores on existing scar or ulcer sites
Open sores (possibly with oozing or crusting) that do not heal, or heal and then reappear
Wart-like growths
Flat sores with crusting
Cutaneous horn
Keratoacanthoma
Carcinoma cuniculatum.
(Hale & Hank 2023; Mayo Clinic 2021)
The lesion will generally range between a few millimetres to several centimetres in diameter and might be inflamed or tender (Oakley 2015).
Dysplasia
Dysplasia is the abnormal growth of a pre-existing lesion, from which cSCCs can develop. Initially, dysplastic keratinocytes above the epidermal basal layer behave abnormally, resulting in a focally thickened stratum corneum (SC); i.e. an actinic keratoses (AK) (Ratushny et al. 2012).
If the atypical keratinocytes demonstrate advancing dysplasia and dysfunction that fully infiltrates the epidermis, this becomes cSCC in situ, Bowen’s disease or intraepidermal carcinoma. A specific histological definition can highlight the lesion’s level of abnormality (Ratushny et al. 2012).
Well-differentiated cSCC’s most closely resemble normal tissue and are more predictable in behaviour than moderately well or poorly differentiated cSCCs, which are the most unpredictable tumours with poorer outcomes (Ratushny et al. 2012).
These less dysplastic, well-differentiated lesions retain some normal tissue function and can produce keratin, which may appear initially as a cutaneous horn (spiky, hard and often painful to the touch) (Ratushny et al. 2012).
Diagnosis and Treatment of Cutaneous Squamous Cell Carcinoma
A cSCC can be diagnosed through physical examination and biopsy if required (Mayo Clinic 2021).
The severity of the cSCC will dictate the appropriate treatment option. cSCCs and other cancers are often categorised using a staging system known as tumour-node-metastasis (TNM), which assesses three aspects of the cancer (EdCaN 2014):
(T) Primary tumour
Size of the tumour
Whether any high-risk features are present (lesion is over a certain size, poor differentiation, growing around a nerve, on the lip or ear)
Whether there is an invasion of facial or skeletal structures
(N) Regional Lymph Nodes
Whether the cancer has spread to lymph nodes
If so, the location, size and number of metastatic tumours
(M) Metastasis
Whether the cancer has spread to distant areas of the body.
Treatment of cSCCs aims to completely remove the tumour in order to avoid recurrent disease or metastasis.
Depending on the patient’s characteristics, low-risk tumours (e.g. well defined, well-differentiated, small, thin and well-sited) can be treated with destructive modalities like curettage, cautery or topical creams.
High-risk tumours require complete excision. Challenging sites, e.g. thick, invasive lesions and lymph node involvement require a referral for comprehensive management (Hale & Hank 2023).
Conclusion
While cSCCs are not usually difficult to treat if addressed early, they have the potential to cause complications if left alone. Therefore, nurses working in all healthcare settings should have up-to-date knowledge of tumour types so that they can promptly identify cSCCs and determine the appropriate treatment for the patient.
Ratushny, V, Gober, MD, Hick, R, Ridky, TW & Seykora, JT 2012, ‘Keratinocyte to Cancer: The Pathogenesis and Modelling of Cutaneous Squamous Cell Carcinoma’, The Journal of Clinical Investigation, vol. 122, no. 2, viewed 3 August 2023, http://doi.org/10.1172/JCI57415
 New
New