An Ausmed and The Nurse Break collaboration brings you this scrolling feed of stories from those on the frontline of the health service!
‘We devised a plan to have a clean nurse and doctor outside the room, and a dirty nurse and doctor inside the room...’
We are fortunate to introduce Amber, who is a graduate nurse on an orthopaedic/trauma ward that has now also become a COVID-19 ward.
I began my graduate nursing program in early February of this year on an orthopaedic and trauma ward. I began to settle into my new career and role as a grad RN, whilst I was watching on the news and my social media the horrors in China and Europe of the COVID-19 crisis. I will be honest, I naively thought: ‘We’re too far away and it won’t come here to Australia’, but as time would tell, I would be mistaken.
A week passed and as Australia received its first cases, and the whole country and its public hospital systems were preparing for an influx; it was revealed that my ward was to be a COVID ward. Immediately we started moving patients and preparing for all we needed to know for COVID-19.
At this point, as every healthcare professional, I was worried. I was worried that my inexperience would make me a weak target for the virus and impair my ability to care for my patients under the circumstances. To the credit of the amazing team of nurses on the floor and my grad support team, I never felt more supported and encouraged in my life.
Thus far my nursing career can be measured up to three months, meaning that nearly two-thirds of my nursing career to date has been related to COVID. Despite this short amount of time, the things that I have learnt clinically and personally through this pandemic are skills and assets that would have taken me many more months, if not years, of experience and exposure to learn.
As a grad working with patients suspected or positive COVID-19 initially was daunting, but I soon learnt that the best way to learn was to ask, to question and to dive straight in and learn from experience. That is exactly what I did. Doing this not only expanded my knowledge, but furthered my skills on problem solving, planning for potential problems, and grouping my care so I could provide as much care as possible with little interaction.
Examples of this include that I was the first nurse on my ward to transfer a COVID patient from ED to our ward, and I had to plan and work out how to keep my PPE clean so I could safely transfer the patient through the hospital. Further, I was the first nurse to have a MET call in a COVID room, where we devised a plan to have a clean nurse and doctor outside the room, and a dirty nurse and doctor inside the room; this in itself provided challenges with communication and safely accessing the equipment that we needed, but we provided the same standard of care under duress conditions.
Ultimately, we as a collective team and profession had to learn as we came across each challenge, which not only made myself and those around me more adaptable but challenged all our initiatives to provide the same standard of care whilst preserving our own personal contact, unnecessary equipment and of course PPE.
As I mentioned before at the start of this crisis I was beyond a nervous wreck, but I cannot deny that this experience has exposed me to a type of nursing that not many grads (or nurses for that matter) ever get exposed too. Although the crisis has devastated the world for many a reason, I always try to see the better in each situation, and I have grown professionally and clinically as a result.
I still believe that everything happens for a reason. I was meant to start nursing this year, with this year 2020 being the ‘Year of the Nurse’, and I was meant to be on this ward and nursing patients potentially or with COVID. I know that nursing will be seen differently after this crisis lifts, for the better I hope, but I know that the nursing that I have done during the COVID-19 pandemic will set me in good stead for the rest of my civilian and military nursing careers.
COVID-19 Graduate Nurse
For many years now Australians have referred to our home as the lucky country.
During the current pandemic, I have truly come to understand and appreciate this sentiment. Our natural borders and swift control measures have (so far) saved our bacon, and as an emergency nurse, I’m truly grateful and proud to live and work in this country. We have avoided the worst of this contagious and deadly virus to date, and our healthcare systems have remained fully functional.
Yet for many healthcare professionals the question remains; when will our turn come, and just how bad is it going to be?
Even if we haven’t yet been inundated with its physical presence, the ‘rona feels like an all-consuming beast. It’s there when I arrive at work, it’s there for every patient assessment, and it’s there as I head home past the ‘STOP if you have a fever’ signs. Then, when I get home, I’m reminded once again. The ‘rona is on the news, in the supermarkets and even in the family Zoom.
COVID-19 isn’t just impacting our physical resources, it’s consuming our mental and emotional energy as well. And while in Australia we’ve been lucky enough to avoid the real physical battle so far, you could say that our minds have already been facing the very real mental battle. I know that I at least certainly feel this way.
As nurses, we often feel an all-consuming responsibility to continue to push harder in times of need, to serve not only our patients but also our families and wider communities as well. Although we know the physical and mental impacts that constant stress can have on our mind and body, we feel an innate responsibility to carry on. We often only think about looking after ourselves at the end of a shift or on days off, but unfortunately, the current situation is making this harder and harder to manage. It’s hard to get space from the pressures of work when the noise of the coronavirus is loud and constant. It’s hard to escape something that’s engulfing and consuming the world’s attention.
As someone who’s experienced burnout before, I’ve noticed these pressures building and have actively decided to focus on how I’m travelling. Through meditation, journaling, exercise and the odd online House-Party, I have been able to remain connected and grateful for our current good fortunes. I know that taking this time out is important to look after myself so that I can be better prepared when I’m most needed. I’m doing everything I can to ensure that when the ‘rona finally comes knocking I have the physical and mental strength to front up against her/his effects.
From personal to professional disaster, written by a senior social worker and academic.
I write alongside my heater in the lounge room as the weather reaches eight degrees centigrade on a dreary and rainy winter-like day in Melbourne, Australia.
Working from home has been a struggle, as I gather myself into some sort of routine by going for a walk, showering and setting up my laptop in an area well insulated in my flat. My housemates are either working a night shift at the hospital attending to COVID-19 demands or have gone home to their families in the countryside due to quarantine restrictions. I have lost a sense of purpose during this time experiencing collective and global anxiety, given the world has lost its way forward as it responds to crisis without forethought about how the world will look when this global health crisis subsides.
Recently, I lost my sessional academic role in teaching social work. This was due to student enrolments decreasing as a result of COVID-19. Sadly, there is no support from the federal government in job seeker payments, which is an injustice for 70% of the higher education workforce who are causal in Australia. However, I applied to access my superannuation early due to losing more than 20% of my income, which was a federal government initiative. Our financial health has taken a battering during the collapse of materialism and a false economy founded on debt and capitalist sentiment.
Fortunately, I continue to work as a mental health clinician in a government department alongside veterans and their families who need support via telehealth. Sharing common and collective concerns over the phone with people has been an empathic unifier as people I partner alongside as a clinician self-manage expectations about timelines and ask you how you are going as a clinician. What a change.
As a social worker in health I am concerned about assessing and redressing the social consequences and social context such as relationships, family, community, culture and spirituality that impact on social issues in our lives.
However, working from home has been difficult, given I am battling with my own experiences of anxiety, mood fluctuations and thought disturbances with a diagnosis of bipolar affective disorder as defined by psychiatry. It can be difficult battling with other inner demons when you are experiencing a similar phenomenon.
The mental health system and its broader intersections with health, education, employment, income security, housing and disability has not been able to cope with the demand and many of us accessing services have felt let down in not attending to our complex grief, loss and trauma. Alongside our formal support system, we have seen the collapse of our informal support system as there has been significant family and relationship conflict due to the physical distancing and quarantine sanctions resulting in a relationship breakdown and discord. Now to deal with my grief without adequate supports.
Despite COVID-19’s detrimental impact on my mental health, I have been able to build inner resilience and sit with my emotions and critical reflections. I have gained a greater sense of self in solitude and am thankful for the positive changes in human behaviour resulting in a more sustainable and just world. We are more than what we produce and consume.
In summary, I think we need to acknowledge privilege and value the contribution of our nurses, doctors and multidisciplinary frontline healthcare workers such as physiotherapists, dieticians, occupational therapists, social workers and administrative staff. You know who you are. Check-in with yourselves. Access work-based mental health support. Check-in with peers and your own multi-disciplinary team, there’s usually a trained counsellor aka social worker. And be kind to yourselves. This will pass and we’re forever grateful to anyone working on the frontline in healthcare.
COVID-19 has not been all that bad. But we have had to sacrifice for great change in how we live, breath and sustain our Earth and human species.
A Social Worker Perspective. The Mental Health and Service User Experience During COVID-19 in Australia: From Personal to Professional Disaster.
Annie works in a large public inpatient psychiatric unit.
With COVID-19 and social distancing, how have you changed how you provide your services to clients in the interim?
I am still going into work, however, now am limited to working on one floor. Many groups are now outside when the weather is suitable and, if not, in open areas. All materials have to be wiped down with disinfectant, general social distancing and hygiene practices are reminded at the start of sessions and, of course, need to be followed.
Family/loved ones are now not attending my creative studio due to visitor restrictions and limitations to group numbers. My day-to-day job role has differed quite a bit as I am picking up other roles that provide group work.
I try to keep the themes ‘connection and safety’ running through the day, so the day will probably start by checking in with the MDT via video chat online, the handovers are also using Microsoft Teams, then I have a coffee and chat in the morning with individuals, facilitate an art therapy group, check in with people after lunch, facilitate a mindful, gentle, physical exercise, and end the day with a mindful exercise. I am also offering staff weekly ‘creative escapes’ as it is hard to switch-off from work as it’s in work, at home and everywhere.
COVID-19 STORY: ART PSYCHOTHERAPIST
I was an ANUM on a general medical ward up until recently.
Then COVID-19 reared its head and I was suddenly an ANUM on a COVID-19 ward, where only confirmed or suspected COVID-19 patients were admitted.
Was I given a choice? No. Why? Because it’s a pandemic. If I was given a choice, would I still be working on a COVID-19 ward? Well, yes, I’m not going to say no. I don’t have any immunity issues, the only thing I suffer from is seasonal asthma.
We are in unprecedented times, never has anything like this been seen in our lifetimes. It’s why I get angry when I see people flouting the lockdown rules, why I get angry when I see people being noncompliant, and thinking that it won’t affect them. It’s not about us. It’s about the people that need protecting – the elderly, the immunosuppressed, the more susceptible and vulnerable people in our society.
It all hit on the weekend, as I held his hand as his eyes glazed over. Patient X was an elderly gentleman admitted for an increased SOB. Because of the SOB and being elderly, he matched the criteria for a COVID-19 swab, which is why he was on our ward, alone, no visitors allowed. He had been stable all morning, so when he requested a shower the primary nurse helped him into the bathroom then left him. She went back and he was on the toilet trying to, well you know. The emergency buzzer goes off.
It takes three loooooong minutes to get into the room because of DRSABC. ‘D’ for danger means making sure we apply PPE properly. We can’t rush these things, even if it means the difference between life and death (a thing that does not sit well with me), but it is a sign of the times.
In the bathroom, Patient X sits on the toilet, still conscious, talking, saying he couldn’t breathe. The primary nurse had given a neb, which I had to run to turn off as we were not equipped to be giving aerosol-generating medications in the ward we were in. I grabbed the patient’s hand whilst asking for more oxygen, a hoist and more hands so that we could at least get the patient back to bed.
There weren’t even enough of us to safely lower him to the floor. I asked the patient whether they had chest pain, he said no. Two minutes later he uttered, ‘I have chest pain’, then his eyes glazed over and he started Cheyne Stoking. By this stage the MET team had arrived, the patient was not for CPR. We lowered him onto the ground, and I was still holding his hand as he took his last breath, there on the bathroom floor.
It hit me, I started to cry. Like an ugly cry. This man, all alone, had not been able to have visitors because of policy. We are the people the patients see, or at least our eyes are. That was the hardest thing in my 15-year career that I have witnessed. The gravity of the situation is there for me now. I will never again take for granted the power of touch for a patient. We are the frontline. We are the faces they will be seeing, not the faces of loved ones.
And if you ever find yourself looking after COVID-19 patients, I implore you to take your time when in the room with them. Chat with the patient, smile with them, cry with them. We might just be that shining light that they need in this awful, horrible time.
Takeaways:
Patients are often isolated and we are the only contact with the outside world, so take that extra five minutes with them. Make the time.
If you find yourself with a patient who is dying, hold their hands because their loved ones can’t.
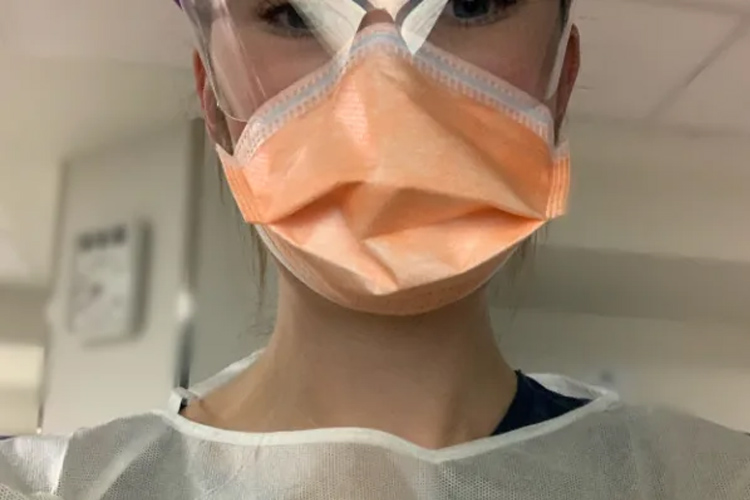
I leave with these words: These are the eyes that greet you when you come to the hospital. If you are unfortunate enough to be tested for COVID-19, then these are the eyes of the healthcare workers who will be caring for you, either on COVID-19 ward or the intensive care unit. These eyes don’t tell you much. But these eyes are smiling with you, laughing with you, crying with you, and are frustrated with and for you. These eyes understand you are at your most vulnerable and isolated.
If you don’t want or need to see these eyes, I implore you to STAY. AT .HOME.
COVID-19 WARD ANUM
(Requested to be anonymous, Dr C is a Medical Registrar in Victoria.)
I’m sure a lot of people have had their plans for 2020 thrown out the window with the COVID-19 pandemic. In the setting of this global pandemic, all of us have got to continue our social distancing to #flattenthecurve.
Fortunately in Australia, our healthcare system is, broadly speaking, fairly robust, accessible and provides quality healthcare to anyone who stumbles into an emergency department or GP practice. And fortunately, we have also managed to flatten the curve sufficiently to avoid pushing our ICU beds and workload beyond maximal capability.
However, anyone who has worked in the public healthcare system knows how closely our hospitals run to capacity even without this coronavirus floating around. If you or a family member has ever had to wait long hours to see a doctor in ‘emergency’ or otherwise, it’s because there are often other patients with acute, urgent medical issues requiring rapid life-saving assessment and treatment.
Long wait times often means prioritising different patients, and can result in people with broken limbs, mental health difficulties, gastro, pain, and many more non-life threatening complaints waiting hours for treatment. This COVID-19 pandemic will prove challenging to Australian healthcare, wait times will inevitably lengthen, hospital capacity will be put under pressure.
The challenges are great, but the difference between becoming Italy or South Korea is mostly in the hands (ideally washed) of the population. Public health is a team effort, understanding the symptoms, avoiding unnecessary social contact, working from home where possible, seeking medical attention when appropriate will also help prevent a future surge in cases and ease pressure on the public health system.
The differing political responses to the pandemic around the world have varying levels of effectiveness from a health and economic standpoint. Policy, laws and rules can only ‘control’ so much. In the end, the responsibility is in our collective hands. The end is not yet in sight unfortunately, there is still a long way to go in controlling the pandemic in terms of going back to the norm.
Stay safe.
Coronavirus: Policy, laws and rules can only ‘control’ so much, in the end, the responsibility is in our collective hands.
Methodically and with great mindfulness, I don my first pair of gloves.
We tried cytotoxic gloves for a few days. The longer cuffs ensured greater coverage, but now we’ve run out. Next is my impervious gown. I continue with my hair cover, then my face shield. It is the beginning of Autumn, but the sun still has bite. Before I have donned my second pair of gloves, I am perspiring. My buddy checks me, and I motion for the driver to come forward. They are playing with their phone, so I wait patiently, breathing deeply and listening to the rosellas chatter in the gumtrees.
‘Good morning. Are you here to be swabbed? What’s your name sir?’ A cough and splutter, I strain to hear his husky voice.
‘Please ensure your window is down and your engine is turned off.’ I make my way behind the vehicle to the driver’s side.
‘In this bundle, there is a work certificate dated for two weeks from today, a list of contact phone numbers, and a COVID-19 Fact sheet. Have you ever been swabbed before?’ He shakes his head. He is teary.
Something suppressed long ago stirs in me and I wonder if he’s worried about dying this year.
‘I am using one swab today. First, I will place it at the back of your throat, then it will go up your nose. It may make you want to gag; your eyes may water, and you may want to sneeze. If you do this, PLEASE ensure you do it in the opposite direction to me sir. Please remain looking ahead at all times.’
He reclines his seat and I approach the car window.
‘Head back, mouth open, tongue out and say “ah”.’ He gags and coughs. ‘Now I will place it in your nostril sir, please try not to scrunch your nose up.’
1, 2, 3, 4, 5, 6… he sneezes, once, twice, three times and I am now dealing with aerosolised COVID. I take two steps back, mindful not to be collected by the car rounding the garden to pick-up their relative from the entrance.
‘You will be contacted in the next week with your results. You must now behave like you are infected and adhere to strict self-isolation rules. You must not leave your home until notified. There are harsh penalties in place for people who violate this order. Do you have any questions?’ He wipes a tear away. He has no questions. ‘You are fine to go sir, take care.’ He thanks me and starts his engine.
I deposit the tube in the pathology bag and move to the bin, where I methodically doff my PPE. I’m thankful for the cool breeze despite the sun, as my perspiration dries, and I begin to don again.
COVID-19 ED Nurse / Drive-Through Clinic
As an ED nurse, my practice has altered slightly...
...as we have had to try and maintain social distancing. I am a kinesthetic type of person, so to not offer someone comfort - hold a hand or cuddle a crying child - has been somewhat difficult for me. Often my co-workers and I debrief – especially if we have experienced sadness, shock or a sudden traumatic event, and often that means a hug in our cohort. We are upskilling in a different emotional way!
To refrain physically means we have had to develop other ways to show our support and convey the warmth someone may require, and also apply this to patient-centred care. This has been a positive learning curve during COVID – amongst many other new skills we seem to be gaining at a rapid rate!
Anxiety and worry understandably exist amongst our team at this time, which brings a level of exhaustion with it. We have had to remain mindful and diligent with our PPE and my hospital has been remarkable in providing constant education and updates on how to handle this pandemic.
The negatives have been woeful, to say the least. I was verbally abused on my way to work at Coles. This occurred even before the measures were put in place to refrain from wearing a uniform to and from my workplace. Anxiety about COVID has manifested in aggression and fear amongst our community, which has been interesting at times. Just trying to smile my way through it!
People need to remember we have families too – some healthcare workers have elderly people at home to care for, immunocompromised people within their circle, and small children. Hugging my kids and turning my face away has become the new norm – but this is not forever!
COVID-19 ED RN
The COVID-19 pandemic has felt surreal for most of us ED nurses.
The ED crew quickly realised how often we touch our patients for good rapport and therapeutic relationships, which is no longer possible due to social distancing, and making physical contact with fellow colleagues for support within the team. We have had to become far more creative with social distancing, such as wearing fun coloured scrub caps for everyone to look at, engaging our patients in different ways other than physical contact and using verbal support - key to lifting each other up.
I have been so grateful for my team and the wonderful people surrounding me and all the extra efforts people are making. We as healthcare workers are much higher risk. Things like the fun scrub caps, people baking snacks, the boys doing MOVID-19 to lift our spirits and remain safe so they can get an adequate seal with their PPE, the zoo live feed on multiple screens in the department, it makes me feel so lucky to be in such a wonderful team!
There has been a huge culture shift with things like scrubs only within the department, social distancing in the tea room and adjusting to ever-changing protocols and plans as the pandemic progresses. The pandemic is bringing out the best in people in that there is SO much education and upskilling preparing for the influx of people getting to know plan after plan. I have also enjoyed just having a bit of quiet time outside of work. With no other commitments outside of work, life is going at a slower pace and it has been a great mental reset for me, allowing me to prepare for what is to come. The world of the unknown has been the hardest part to navigate: new policies and procedures coming in every day, change is always difficult but we are helping educate and assist each other.
My biggest wishes for the community:
Don’t panic.
Utilise the COVID-19 hotline as often as you need for questions.
Don’t wear gloves all day! Wash your hands, please!
Stay at home and please social distance.
Don’t be afraid to ask questions, there are so many resources to get the answers you’re looking for and to assist you to be as comfortable as possible through this process.
(PS: Don’t steal personal protective equipment from hospitals – you are safe at home and we need it.)
To all my fellow healthcare workers, orderlies, security and the rest of our beautiful community.
Not knowing the answer right away is ok, don’t be afraid to ask your seniors, utilise hotlines and ask your family. Look after yourself, eat, don’t overwork and make sure you enjoy downtime while you can. We can all rely on each other for love and support! My personal advice is to avoid the news and watch the live feed of the pandas at the zoo. We have them going in our department 24/7, and boy it lifts your spirits!
Nurse within Major ED: Working Frontline with COVID-19
An Ausmed and The Nurse Break collaboration brings you this scrolling feed of stories from those on the frontline of the health service!
Want to be featured? Go HERE to learn more, or email submissions to thenursebreak@gmail.com.
We want you, whether you are a medical, paramedic or nursing student on placement, a ward clerk in a COVID-19 ward or ED, an ICU doctor, nurse, physiotherapist, social worker, paramedic, pathologist, orderly….an aged care support worker, a pharmacist, a dentist.
Topics
For Teams
Assign to your staff
Assign mandatory training and keep all your records in-one-place.
 New
New