Increased intracranial pressure is a medical emergency with the potential for a variety of serious complications, including death. It requires urgent treatment (Johns Hopkins Medicine 2016).
What is Increased Intracranial Pressure?
Increased intracranial pressure (ICP) occurs when pressure is elevated inside the cranial vault, which contains three components:
The brain
Cerebrospinal fluid (CSF)
Blood.
(Pinto et al. 2022)
The cranial vault is often described using the Monro-Kellie doctrine - the hypothesis that the cranial vault is similar to a fixed box, where any change in the volume of its contents leads to an increase in pressure (Nickson 2020).
Using this hypothesis, the three components of the cranial vault can be considered to have a fixed total volume; therefore, if one of the three components (brain matter, cerebrospinal fluid or blood) increases in volume, there is little capacity for the total intracranial volume to increase. This results in raised intracranial pressure, which can have a variety of serious consequences (Pinto et al. 2022; AMBOSS 2022).
Typically, when a person is in the supine position, the pressure inside the cranial vault is at or below 15 millimetres of mercury (mmHg) in adults, and less in children. ICP adjusts when the position of the head changes relative to the body, and in response to physiological processes such as sneezing and coughing (AMBOSS 2022).
An ICP of at or above 20 mmHg indicates pathologic intracranial hypertension (AMBOSS 2022).
Causes of Increased Intracranial Pressure
Factors that can increase the volume of the cranial vault, and consequently lead to raised ICP, include:
Hydrocephalus - an increase in cerebrospinal fluid (e.g. caused by increased CSF production or a choroid plexus tumour)
A decrease in the reabsorption of cerebrospinal fluid (e.g. caused by obstructive hydrocephalus or meningeal inflammation)
Intracranial haemorrhage (bleeding) or haematoma
Swelling in the brain
Trauma to the head or brain
Brain tumour or abscess
Certain infections (encephalitis or meningitis)
Intracranial hypertension, which when idiopathic, often affects young, overweight females aged between 20 and 45 years
Stroke
Increased venous pressure (e.g. caused by cardiac failure)
(Johns Hopkins Medicine 2016; Pinto et al. 2022; AMBOSS 2022; NORD 2018; Nickson 2020)
Signs and Symptoms of Increased Intracranial Pressure
The symptoms of increased ICP are known to be non-specific and might resemble other conditions (Carey et al. 2022).
The most characteristic symptom of increased ICP is a severe, unbearably painful headache. It may awaken the patient at night and not be relieved by analgesic medicines (NORD 2018).
A headache indicative of increased ICP might also be exacerbated by moving the head or coughing and is often associated with an altered mental state (Willacy & Tidy 2021).
Other potential symptoms of increased ICP include:
Nausea and vomiting
Altered mental state, e.g. irritability, impaired decision-making, abnormal social behaviour
Vision changes, e.g. blurry vision, double vision, photophobia, papilloedema (swelling of the optic disc)
Weakness and lethargy
Pupillary changes, e.g. irregularity or dilatation in one eye
Motor changes
Seizures
Hypertension
Irregular respiration
Bradycardia
Widened pulse pressure (a wide gap between systolic and diastolic blood pressures)
Slow, irregular pulse
Macrocephaly, bulging fontanel and sunset eye sign (in infants).
(Pinto et al. 2022; Willacy & Tidy 2021; AMBOSS 2022; Carey et al. 2022)
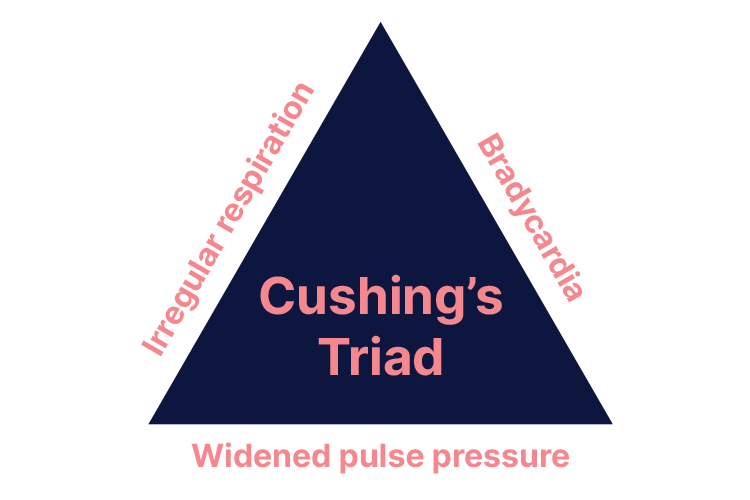
Cushing’s Triad
Cushing’s triad is a set of three clinical signs indicative of increased ICP. These signs are:
Bradycardia
Irregular respiration
Widened pulse pressure.
(Mauldin et al. 2020)
Cushing’s triad occurs when increased ICP decreases the cerebral blood flow significantly. A response is triggered that increases arterial pressure in order to overcome the increased ICP (Dinallo & Waseem 2020).
At this point, if treatment does not occur to stabilise the ICP, herniation of the brain stem and occlusion of the cerebral blood flow can occur with dire consequences (Dinallo & Waseem 2020).
Complications of Increased Intracranial Pressure
Potential complications of increased ICP include:
Coma
Optic atrophy
Seizures
Stroke
Neurological damage
Brain herniation, which is potentially fatal and preceded by Cushing’s triad
Death.
(Johns Hopkins Medicine 2016; Pinto et al. 2022)
Diagnosing Increased Intracranial Pressure
Increased ICP may be diagnosed using:
Medical history and physical examination, including a neurological exam
Lumbar puncture (spinal tap) to measure the pressure of the cerebrospinal fluid
CT scan
MRI scan.
(Johns Hopkins Medicine 2016)
As a general rule, any patient presenting with a headache, vomiting and blurred vision should undergo head imaging to rule out increased ICP. Furthermore, those who have experienced a severe traumatic brain injury presenting with a Glasgow Coma Scale score of three to eight should undergo ICP monitoring in accordance with severe traumatic brain injury management guidelines (Pinto et al. 2022).
Management of Increased Intracranial Pressure
The main principles of managing increased ICP should be:
Raising mean arterial pressure in order to maintain cerebral perfusion pressure
Addressing the underlying cause
Lowering the ICP
Preventing secondary injury.
(Pinto et al. 2022; AMBOSS 2022)
Note: Always ensure ICP readings are correct and rule out measurement errors (Nickson 2020).
If the patient requires acute resuscitation and stabilisation, always follow the ABCDE assessment approach and ensure airway management, ventilation and circulation are prioritised (Pinto et al. 2022; AMBOSS 2022).
Once the patient is stabilised, management of increased ICP in the critically ill patient in an intensive care environment might include:
Removal of any artefacts causing the raised ICP
Maintaining adequate oxygen delivery
Maintaining adequate cerebral perfusion pressure (CPP = MAP – ICP) using fluid, inotropes and vasopressors
Elevating the head of the bed to optimise the venous return from the brain
Avoiding cerebral vasoconstriction by monitoring PaCO2 levels
Decreasing cerebral metabolic rate (the amount of oxygen and glucose the brain needs) - this may be achieved through sedation, analgesia, paralysis, avoiding hyperthermia, treating seizures, and barbiturate coma
Administering osmotherapies such as mannitol or hypertonic saline to reduce intracranial pressure (to draw oedema out of the cerebral tissues to decrease ICP)
Considering hypothermia (in some situations, only with the goal of reducing cerebral metabolism)
Surgical techniques such as insertion of an extraventricular drain (EVD), evacuation of haematoma and/or decompressive craniotomy. (It’s important to note that decompressive craniotomy remains contentious following the DECRA trial. More on this topic can be found here.)
(Nickson 2020)
Note: A study by Monash University (n.d.) discourages the use of albumin in the resuscitation of critically ill patients with a traumatic brain injury, as it may increase the risk of mortality.
Remember:
Any changes in the volume of the cranial vault (blood, CSF or brain tissue) leads to an increase in pressure
Any patient presenting with a headache, vomiting and blurred vision should undergo head imaging to rule out increased ICP
Cushing’s triad is a set of three clinical signs indicative of increased ICP
Increased intracranial pressure is a medical emergency with the potential for a variety of serious complications, including death.
Test Your Knowledge
Question 1 of 3
What is the typical intracranial pressure in adults?
 New
New