Hip fractures are potentially catastrophic injuries, particularly in older adults, and are associated with death, disability and loss of independence (Davenport 2021).
Approximately 19,000 people fracture their hip every year in Australia (AIHW 2018). Incidences of hip fractures appear to be increasing as the Australian population ages (Leung et al. 2023).
What is a Hip Fracture?
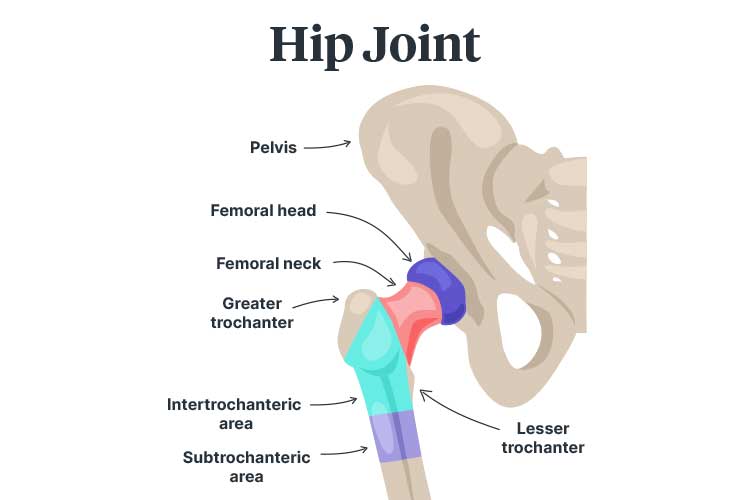
The head of the femur (thigh bone) fits into a socket in the pelvis to form the hip joint (Fischer & Gray 2020).
A hip fracture occurs when the top of the femur cracks or breaks (Fischer & Gray 2020).
Areas where the femur may fracture include:
The femoral head
The femoral neck
The intertrochanteric area (between the greater and lesser trochanters)
The subtrochanteric area (under the greater and lesser trochanters).
(Fischer & Gray 2020)
Femoral neck fractures are the most common, accounting for about 56% of injuries (AIHW 2018).
Hip fractures are classified according to the extent of displacement:
Non-displaced fractures occur when the femur cracks without separating
Minimally displaced fractures occur when the femur shifts along or away from the fracture
Displaced fractures occur when part of the bone detaches completely.
(Harvard Health Publishing 2020)
Hip fractures are potentially life-threatening, with approximately 8% of injuries resulting in death within 30 days (Leung et al. 2023). Many of those who survive experience permanent impairments to their daily functioning (Mayo Clinic 2022).
Potential consequences of hip fractures and associated immobility include:
Hip fractures are most common in older adults over 65 and may indicate poor underlying health (ACSQHC 2023).
Causes of Hip Fractures
Most hip fractures are caused by falls (ACSQHC 2023). In 2015-2016, 93% of new hip fractures were fall-related, with 87% being only minimal trauma falls (AIHW 2018).
Furthermore, hip fractures account for 20% of all fall-related hospital admissions (ACSQHC 2017).
Other potential causes include:
Severe impact (e.g. a car accident)
Twisting or tripping
Standing or walking (in cases of severe bone weakness).
(Mayo Clinic 2022; Fischer & Gray 2020)
Risk Factors for Hip Fractures
Age, as bone density and muscle mass decrease naturally over time
Vision and balance issues
Being female, as the reduction in oestrogen caused by menopause increases bone density loss
Certain medical conditions that cause bones to weaken, including endocrine disorders and intestinal disorders
Neurological conditions, which may increase the risk of falling
Low blood sugar or hypotension, which may increase the risk of falling
Inadequate calcium and vitamin D intake, which reduces peak bone mass
Lack of physical activity, which may lead to frailty
Smoking and alcohol use, which may disrupt bone building and maintenance processes
Being an Aboriginal or Torres Strait Islander person.
(Mayo Clinic 2022; ACSQHC 2023)
Symptoms of Hip Fractures
Acute pain in the groin and upper thigh
Bruising and swelling near the hip
Difficulty standing
Difficulty bearing weight on the injured leg
Difficulty moving, lifting or turning the upper leg or knee
A noticeable difference in length between legs (the injured leg may look shorter than the other leg)
The injured leg turning outwards.
(Fischer & Gray 2020; NHS 2023)
Treating Hip Fractures
Most hip fractures require surgery. This should ideally be performed within 48 hours of hospital presentation. Surgery involves using internal fixations to hold the bone together. In some cases, patients require a partial or complete hip replacement (NHS 2023; Mayo Clinic 2022).
Preventing Hip Fractures
Falls prevention is especially important after an initial hip fracture.
Maintaining bone strength through regular exercise and adequate calcium and vitamin D intake.
(Harvard Health Publishing 2020)
Falls prevention is especially important after an initial hip fracture, as people who have experienced one hip fracture are at increased risk of experiencing another (Sheikh et al. 2019).
In 2023, the Australia Commission on Safety and Quality in Health Care released the updated Hip Fracture Care Clinical Care Standard. This standard aims to improve assessment and management of hip fractures and reduce the risk of subsequent hip fractures (ACSQHC 2023).
The standard contains seven quality statements:
1. Care at Presentation
Patients who present with a suspected hip fracture should receive prompt assessment and management, including diagnostic imaging, pain relief and assessment of cognition, nutrition and frailty (ACSQHC 2023).
2. Pain Management
Patients with hip fractures should undergo regular pain assessments to ensure they are receiving adequate pain relief. Pain relief may include multimodal analgesia and nerve blocks.
Pain assessments should be performed regularly as part of routine nursing. Additionally, they should be performed:
Upon presentation
Within 30 minutes of initial analgesia provision
Every hour until the patient is settled in the ward.
(ACSQHC 2023)
3. Orthogeriatric Model of Care
Hip fracture treatment should be based on an orthogeriatric model of care, which is defined in the Australian and New Zealand Guideline for Hip Fracture Care. A coordinated interprofessional approach should be used recognise and manage malnutrition, frailty, cognitive impairment and delirium (ACSQHC 2023).
4. Timing of Surgery
Patients should undergo surgery within 36 hours of presentation to hospital (ACSQHC 2023).
5. Mobilisation and Weight-Bearing
Patients should be mobilised starting the day of, or the day after, surgery and then at least once per day (unless there are contraindications). Patients should bear weight on the affected leg depending on their tolerance (ACSQHC 2023).
6. Minimising Risk of Another Fracture
Prior to discharge, patients should be given a falls and bone health assessment and management plan. Prevention strategies may include exercises to improve muscle strength and balance, as well as bone protection medicines if required. Patients may also be referred for secondary fracture prevention (ACSQHC 2023).
7. Transition From Hospital Care
Prior to discharge, patients and their carers should work with clinicians to develop an individualised care plan containing:
Mobilisation activities
Post-injury functioning
Wound care
Pain management
Nutrition
Fracture prevention strategies
Medicine changes
New medicines
Rehabilitation services and equipment.
Upon discharge, a copy of this plan should be forwarded to the patient, their general practitioner and any ongoing clinicians and care providers (ACSQHC 2023).
(ACSQHC 2023)
Test Your Knowledge
Question 1 of 3
What is the recommended timeframe for surgical treatment of a hip fracture?
Sheikh, H Q, Hossain, F S, Khan, S, Usman, M, Kapoor, H & Aqil, A 2019, ‘Short-Term Risk Factors for a Second Hip Fracture in a UK Population’, European Journal of Orthopaedic Surgery & Traumatology, vol. 29, no. 5, viewed 20 February 2024, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6570666/
 New
New