Abnormal posturing is an indicator of extremely severe damage to the central nervous system.
While the recovery outlook of those displaying abnormal posturing is poor, being able to recognise the characteristic signs of severe brain trauma means the patient will receive emergency treatment as quickly as possible and have the best chance of survival (Denslow & Flint Rehab 2021).
What is Abnormal Posturing?
Abnormal posturing is used to describe an involuntary, abnormal body posture that occurs in response to a noxious (pain-causing) stimulus (Denslow & Flint Rehab 2021; Knight & Decker 2023).
In most cases, abnormal posturing is caused by severe trauma to the central nervous system (Biggers & Allen 2021).
Abnormal posturing is a medical emergency indicative of very serious injury, and the patient will likely be unconscious. Most patients displaying abnormal posturing will need to be ventilated and admitted to the intensive care unit (Gill & Frothingham 2018).
Note: Abnormal posturing is pathological. It is not the same as slouching or having ‘poor posture’ (Gill & Frothingham 2018).
Decerebrate posturing, also known as extensor posturing (AMBOSS 2023), is characterised by the following body position:
Arms and legs held straight out and rigid
Neck and head arched backwards
Toes pointed downward
(Weiss 2021)
In severe cases of decerebrate posturing, the patient might also experience opisthotonos (severe muscle spasms of the neck and back) (Weiss 2021).
Decerebrate posturing may occur on one or both sides of the body or in the arms only. It’s also possible for one side of the body to display decerebrate posturing and the other side to display decorticate posturing (Weiss 2021).
Decerebrate posturing is most commonly associated with injury to the distal brainstem or pons at or below the level of the red nucleus (AMBOSS 2023).
Decorticate Posturing
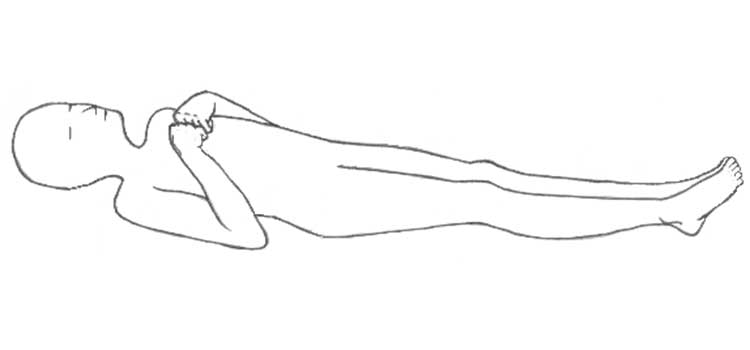
Decorticate posturing, also known as flexor posturing (AMBOSS 2023), is characterised by the following body position:
Arms bent and stiff
Legs held straight out
Clenched fists
Arms bent in towards the core of the body
Fingers and wrists bent and held on the chest
(Weiss 2021)
Decorticate posturing is caused by injury to the proximal brainstem (nerve pathway between the spinal cord and brain), proximal to the level of the red nucleus. It can occur on one or both sides of the body and is more likely to affect only one side of the body than decorticate posturing (Weiss 2021; AMBOSS 2023; Denslow, E & Flint Rehab 2021)
Decorticate posturing is rarer than decerebrate posturing and has a higher survival rate, but is still indicative of very serious injury (Denslow, E & Flint Rehab 2021).
Glasgow Coma Scale
On the Glasgow Coma Scale, decerebrate and decorticate posturing fall under the motor response category:
Behaviour
Rating
Score
Eye Opening Response
Opens eyes spontaneously
4
Opens eyes in response to speech and sound
3
Opens eyes in response to painful stimuli
2
Does not open eyes
1
Verbal Response
Oriented to time, person and place
5
Confused and disoriented
4
Utters incoherent words
3
Incomprehensible sounds
2
Makes no sounds
1
Best motor response
Obeys two-part requests
6
Localises to painful stimuli
5
Flexion/withdrawal from painful stimuli (normal flexion to pain)
4
Decorticate posturing (abnormal flexion from painful stimuli)
3
Decerebrate posturing (extension to painful stimuli)
2
Makes no movement
1
(Adapted from AMBOSS 2023; Moyle 2021)
As seen above, decorticate posturing (abnormal flexion to pain) and decerebrate posturing (extension to pain) score three and two points, respectively, for motor response.
Treatment of Abnormal Posturing
Abnormal posturing is an emergency requiring immediate intervention in order to stabilise the patient. Most patients who experience abnormal posturing will be in a comatose state and, therefore, will have difficulty maintaining their airway and cardiorespiratory system. Consequently, the patient will urgently require mechanical ventilation and admission into intensive care (Knight & Decker 2023; Weiss 2021; Denslow, E & Flint Rehab 2021)
Once the patient stabilises, they will be physically examined, and their medical history will be investigated. Family members may be asked questions about:
Whether there is a history of head injury
Whether there is a pattern to posturing episodes
Whether the posturing has stayed the same
When the symptoms started
Whether the patient experienced any other symptoms before or during the posturing.
(Weiss 2021; Mount Sinai 2023)
Other investigations may also be performed, including:
Blood or urine tests to detect drugs or toxic substances and measure chemicals and minerals in the body
ECG scan
X-ray
Cerebral angiography
MRI scan
CT scan
Intracranial pressure monitoring
Lumbar puncture to collect cerebrospinal fluid.
(Weiss 2021; Mount Sinai 2023)
Specific treatments will depend on the underlying cause of the posturing (Denslow, E & Flint Rehab 2021).
Prognosis
Abnormal posturing is associated with very high mortality rates. Following a head injury, only 37% of patients displaying decorticate posturing and 10% of those displaying decerebrate posturing will survive (Knight & Decker 2023).
Paediatric patients tend to have an increased rate of survival, with an estimated mortality rate of between 10 to 13% (excluding cases of very severe injury) (Knight & Decker 2023).
Overall, factors that appear to increase the risk of survival in TBI include:
Younger age
Admission within six hours of injury
Extradural haematoma
(Knight & Decker 2023)
In cases of hypoxic brain injury, those who still have a GCS motor score of under four after one day post-injury have very little chance of regaining independence. Abnormal posturing caused by gunshot wounds to the head indicates a poor chance of recovery (Knight & Decker 2023).
Those who do survive after experiencing abnormal posturing may sustain permanent damage to the brain. Potential complications include:
 New
New