 New
New Fetal Alcohol Spectrum Disorder (FASD): The Dangers of Drinking During Pregnancy
CPDTime.
3m
Published: 05 July 2021



Published: 05 July 2021
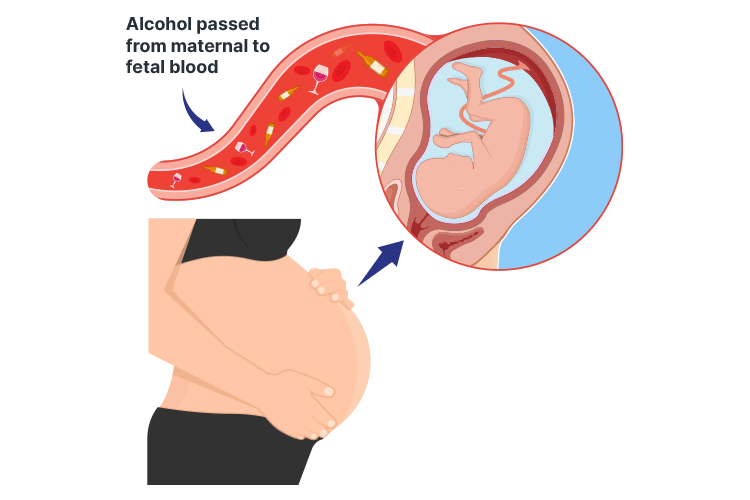
Prenatal alcohol exposure. Is there a safe limit?
Drinking alcohol prior to conception and during pregnancy can have significant adverse outcomes for the fetus, including miscarriage, premature birth or stillbirth (The Women’s 2018).
When a pregnant woman drinks, alcohol enters the fetus’s bloodstream via the placenta and may impact the development of the fetus’s brain or other organs (The Women’s 2018; DoH 2018).
There is no known safe level of alcohol use during pregnancy, and it’s not possible to predict the extent to which a fetus will be affected by alcohol. For this reason, the safest option is to completely avoid alcohol prior to conception and during pregnancy (The Women’s 2018).
Fetal alcohol syndrome disorder (FASD) is known to be associated with persistent physical and neurodevelopmental abnormalities (Vaux et al. 2016). FASD crosses all socioeconomic groups and affects all races and ethnicities (DoH 2018).
It’s a condition that is both disabling and entirely preventable.
The term fetal alcohol spectrum disorder (FASD) describes a range of adverse effects that may occur following alcohol exposure during the prenatal period. These effects include physical, mental, behavioural and learning disabilities, and may have lifelong implications (Better Health Channel 2019).
While the prevalence of FASD in Australia is difficult to determine, it is estimated that up to 2% of babies may be born with a type of FASD (DoH 2018).
In order to be diagnosed with FASD in Australia, there must be evidence of prenatal alcohol exposure, and the individual must also display severe impairment in at least three of the following neurodevelopmental domains:
(Bower & Elliott et al. 2016)
From here, there are two subcategories of an FASD diagnosis:
(Bower & Elliott et al. 2016)
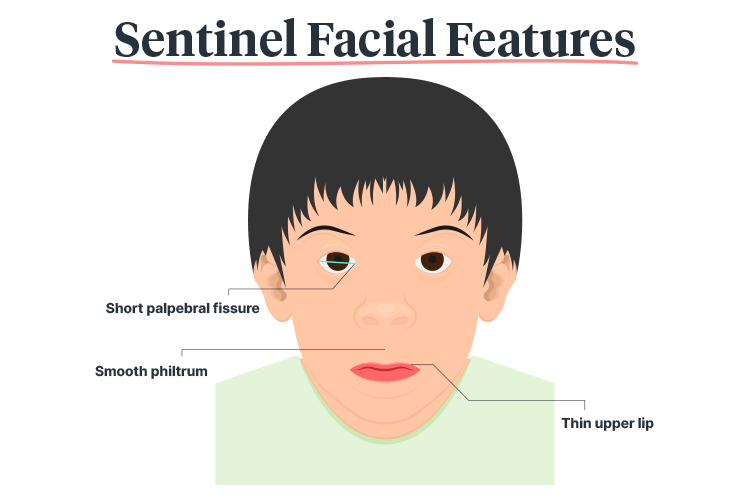
These sentinel facial features include:
(Bower & Elliott et al. 2016)
As Mitchell et al. (2018) suggest, nurses and midwives are in an ideal position to talk to couples of reproductive age about the dangers of alcohol use in pregnancy.
In some cases, the prevention of alcohol-exposed pregnancies requires skilful conversations and appropriate follow up to be clinically effective.
The fact remains that the all-important first step in reducing the incidence of FASD begins by asking about alcohol consumption and advising women about its effects during pregnancy.
Just as with other forms of lifestyle advice, however, talking alone is often not enough to bring about a behavioural change. Wherever possible, women planning a pregnancy should also be assisted to stop their alcohol consumption and be offered further support, referral, follow up and treatment where needed.
Make sure that the following guidance is provided:
(Williams & Smith 2015; Heath 2019)
Remember that there is no wrong time to screen or educate patients who may be at risk of drinking during pregnancy (Heath 2019).

As Eguiagaray et al. (2016) suggest, there is currently a pressing need for greater openness with mothers to challenge the stigma of drinking alcohol during pregnancy.
Drinking in pregnancy is clearly a highly emotive issue that requires sensitive and careful management. On the one hand, delivering alcohol brief interventions (screening the patient for alcohol and drug use) (Rodgers 2018) at the first antenatal appointment is more likely to produce results, but it can also threaten to damage the relationship between midwife and mother.
Recognising this, Doi et al. (2015) suggest that when training midwives to screen and deliver alcohol brief interventions, special attention is needed to improve person-centred communication skills in order to overcome any barriers associated with discussing alcohol use.
Eguiagaray et al. (2016) go further by suggesting that guidelines for media reporting should also be revised to discourage stigmatising mothers, and that media articles should also consider the role that government, non-government organisations and the alcohol industry itself could play in improving FASD shame.
Alongside these suggestions are calls for more education and counselling to raise awareness of FASD. Larcher and Brierley (2014) recommend that this could also helpfully be part of a wider public health and social policy initiative on reducing alcohol consumption.
Supportive strategies include:
(Heath 2019)
Question 1 of 3
True or false: It is safe to consume alcohol while trying to conceive.


Ausmed Education is a Trusted Information Partner of Healthdirect Australia. Verify here.