 New
New Care of Central Venous Catheters
CPDTime.
9m
Published: 02 May 2023


Published: 02 May 2023
Central venous catheters are highly prevalent in critical care environments and pose a number of serious risks to patients. They require thorough care and assessment by healthcare workers.
A central venous catheter (CVC), also known as a central line or central venous access device, is a thin, flexible tube used to deliver treatment or draw fluids (ATS 2019).
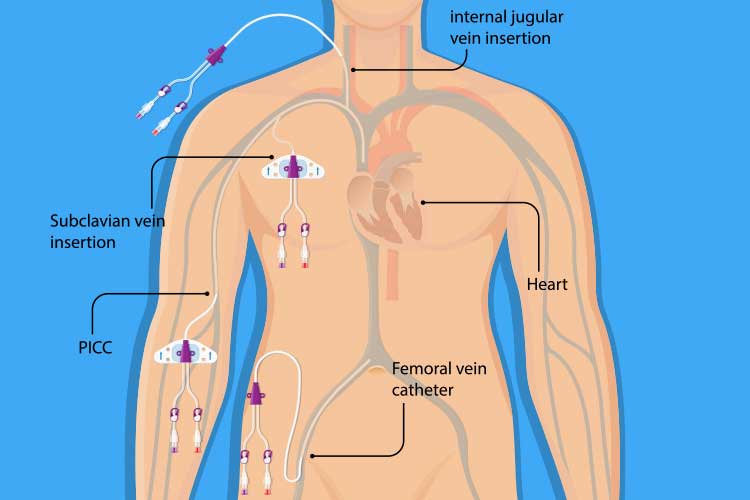
A CVC is inserted through the patient’s skin and into their body through a peripheral vein or proximal central vein - usually either the internal jugular (neck), femoral vein (groin) or subclavian vein (upper chest). The tip of the CVC should lie on the right side of the heart within either the superior vena cava, the right atrium or the inferior vena cava (Kolikof et al. 2022).
Many CVCs are multi-lumen catheters, meaning the catheter has multiple (generally two or three) internal channels that can deliver several medications to the patient simultaneously (usually dispensing each fluid at a slightly different point along the catheter) (LHSC 2014).
(Note: Always check whether medications are compatible before ‘piggybacking’ them in the same lumen.)
A peripherally inserted central line (PICC line) is a type of long CVC that is inserted into one of the large veins above the bend of the patient’s elbow, with the tip resting in the same place as a regular CVC (Macmillan Cancer Support 2021).
CVC insertion is a common procedure, with approximately 15,000 devices being inserted every year in New South Wales intensive care units alone (CEC 2015). However, it does pose a variety of risks (Kolikof et al. 2022).
For this reason, it is important to have a thorough understanding of how to care for a patient with a CVC.
In comparison to an intravenous catheter (IV), a CVC is longer, larger and able to stay in situ long-term due to the greater tolerance of large veins. As a result, a CVC provides convenience to not only the clinician treating the patient, but also to the patient, as it prevents trauma from repeated needle and catheter insertion (ATS 2019; ACS 2023).
Reasons for using a CVC may include:
(ATS 2019; ACS 2023)

When caring for a patient with a CVC in situ, you need to ensure the safety and security of the catheter, have an understanding of which medications are compatible when performing safety checks, and be able to identify any infections of the insertion site.
(Tsotsolis et al. 2015; Smith & Nolan 2013; Queensland DoH 2015; ACI 2021)
CVC insertion is prone to a variety of complications including insertion issues, incorrect placement, internal injury and infections (Patel et al. 2019).
The experience level of the physician responsible for inserting the CVC is shown to be a crucial factor in the occurrence of complications; insertion by an individual who has performed over 50 catheterisations is half as likely to result in a mechanical complication as one performed by a less-experienced counterpart. Furthermore, unsuccessful catheterisation attempts preceding the insertion will also increase the likelihood of complications (Tsotsolis 2015).
Possible complications include, but are not limited to:
(ATS 2019; ACS 2023; ACI 2021)

The risk of complications, some potentially serious, means CVC safety checks are imperative. You must always ensure medication safety and compatibility are maintained, and the line is secure and safe from harm.
Question 1 of 3
True or false: A CVC can stay in situ for longer than an IV.


Ausmed Education is a Trusted Information Partner of Healthdirect Australia. Verify here.